
3D Views of the Sacroiliac Joint
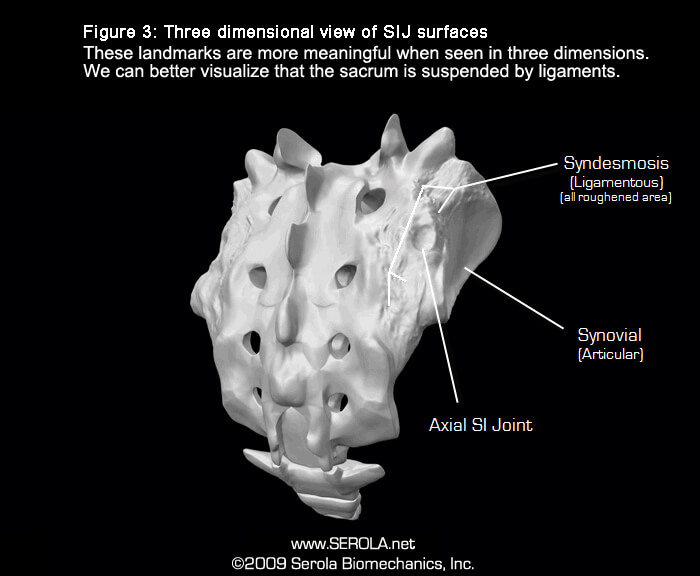
There are two regions to the sacroiliac joint: synovial (articular) and syndesmotic (ligamentous) [1] [2]p27 [3]p266. Most research on the sacroiliac joint is done on the synovial region. Other than the works of Sashin [4] DeJarnette[5]p143-209, Rosatelli et al. [1], DonTigny [6], Vukicevic et al.[7] and Cusi [8, 9], few articles discuss the syndesmosis region.
There is a ridge on the iliac articular surface that runs the length of the joint surface and a corresponding depression on the sacral articular surface into which the ridge fits [4, 10, 11]. This ridge and depression arrangement reflects sacroiliac joint movement.
Rosatelli et al. [1] found that the ridge and depression also occur in the syndesmosis region, although they form later in age. They found that the strong interosseous ligament consists of short, tough bands which pass in different directions from the sacrum to the ilium, evidenced by a roughened area that is quite distinct from the relatively smooth articular region [4]. The interosseous ligament takes up most of the space between the ilium and sacrum, holding them together yet maintaining space between them.
Analogous to the articular region, the ilia has a convex surface and the sacrum has a corresponding concavity with similar ridges and depressions, but smaller and with less roughening, although extensive [1]. The severity of the ridges and depressions were age related, being worse in the older specimens and were present in 100% of those over 55 years of age. Unlike the articular region, the syndesmosis region demonstrated internal ossification, most markedly in the central region, effectively fusing the sacrum and ilium at that point. Ossification occurred in 60% of the specimens over 60 years of age.
The appearance of ridges and grooves at both the articular and syndesmosis regions demonstrates that both regions undergo similar compressive movements. Therefore, it is unlikely that compression could occur at the articular area without also occurring at the syndesmosis. Within the syndesmosis, the retro-articular space between the sacrum and ilium is filled with the interosseous and short posterior ligaments. Within these ligaments are nerves, blood and lymph vessels, fat, elastic and connective tissues [4] [1], and the axial sacroiliac ligament which, due to the low ratio of collagen and high ratio of connective tissue and blood vessels, is one of the weakest ligaments in the body, as measured by failure load and failure stress [12]. If compression is generated by body weight, especially during heavy lifting, it could conceivably decrease blood and lymph flow and damage the tissues within the syndesmosis. Therefore, degenerative changes in both regions and potential crushing of the vessels in the syndesmosis region suggest that these compressive changes in both regions are not normal developments but, rather, the result of dysfunction after injury.
The movement pattern of the sacroiliac joint is complicated due to the shape of the sacrum and the orientation of the articular surfaces, which form a modified saddle joint. The superior portions of the sacral surface face posterolaterally and the inferior portions face anterolaterally [13-16]. Thus, the orientation of the upper and lower articular surfaces denotes a twisting motion; in effect, they curl around the lateral edges of the sacrum. As a pivot point, the axial sacroiliac joint is at the center point where the joint twists from a posterior orientation to an anterior orientation, at the level about S2. Please see Facets Curl Around the Sacrum.
References:
- Rosatelli, A.L., A.M. Agur, and S. Chhaya, Anatomy of the interosseous region of the sacroiliac joint. The Journal of Orthopaedic and Sports Physical Therapy, 2006. 36(4): p. 200-8.
- Bogduk, N., Clinical Anatomy of the Lumbar Spine and Sacrum. 2005: Elsevier Churchill Livingstone.
- McMinn, R.M.H. and R.T. Hutchings, Color Atlas of Human Anatomy. 1977, Chicago: Medical Publishers, Inc.
- Sashin, D., A critical analysis of the anatomy and the pathologic changes of the sacro-iliac joints. The Journal of Bone and Joint Surgery, 1930. 12: p. 891.
- DeJarnette, M., Sacral Occipital Technic Notes 1984. 1984: self published.
- DonTigny, R.L., Mechanics and Treatment of the Sacroiliac Joint. J Manipulative Physiol Ther, 1993. 1: p. 3-12.
- Vukicevic, S., et al., Holographic analysis of the human pelvis. Spine, 1991. 16(2): p. 209-14.
- Cusi, M., SPECT-CT on patients with a clinical diagnosis of failure of load transfer of the sacro-iliac joint, in 7th Interdisciplinary World Congress on Low Back & Pelvic Pain. Effective Diagnosis and Treatment of Lumbopelvic Pain. 2010: Los Angeles, CA. p. 291-296.
- Cusi, M., et al., Metabolic disturbances identified by SPECT-CT in patients with a clinical diagnosis of sacroiliac joint incompetence. Eur Spine J, 2013. 22(7): p. 1674-82.
- Bowen, V. and J.D. Cassidy, Macroscopic and microscopic anatomy of the sacroiliac joint from embryonic life until the eighth decade. Spine, 1981. 6(6): p. 620-8.
- Haldeman, S., et al., eds. Principles and Practice of Chiropractic. 3rd ed. 2005, McGraw-Hill.
- Bechtel, R., Physical characteristics of the axial interosseous ligament of the human sacroiliac joint. Spine J, 2001. 1(4): p. 255-9.
- Solonen, K.A., The sacroiliac joint in the light of anatomical, roentgenological and clinical studies. Acta Orthopaedica Scandinavica. Supplementum, 1957. 27(Suppl 27): p. 1-127.
- Dijkstra, P.F., A. Vleeming, and R. Stoeckart. Complex Motion Tomography of the Sacroiliac Joint and an Anatomical and Roentgenological Study. in First Intedisciplinary World Congress on Low Back Pain and Its Relation to the Sacroiliac Joint. 1992. San Diego, CA.
- Snijders, C.J., Transfer of Lumbosacral Load to Iliac Bones and Legs: Part 1 – Biomechanics of Self-Bracing of the Sacroiliac Joints and its Significance for Treatment and Exercise. Clinical Biomechanics, 1993a. 8: p. 285-294.
- Vleeming, A., et al., The role of the sacroiliac joints in coupling between spine, pelvis, legs and arms., in Movement, Stability, and Low Back Pain, A. Vleeming, et al., Editors. 1997, Churchill Livingstone. p. 53-71.