
Sacroiliac Ligaments
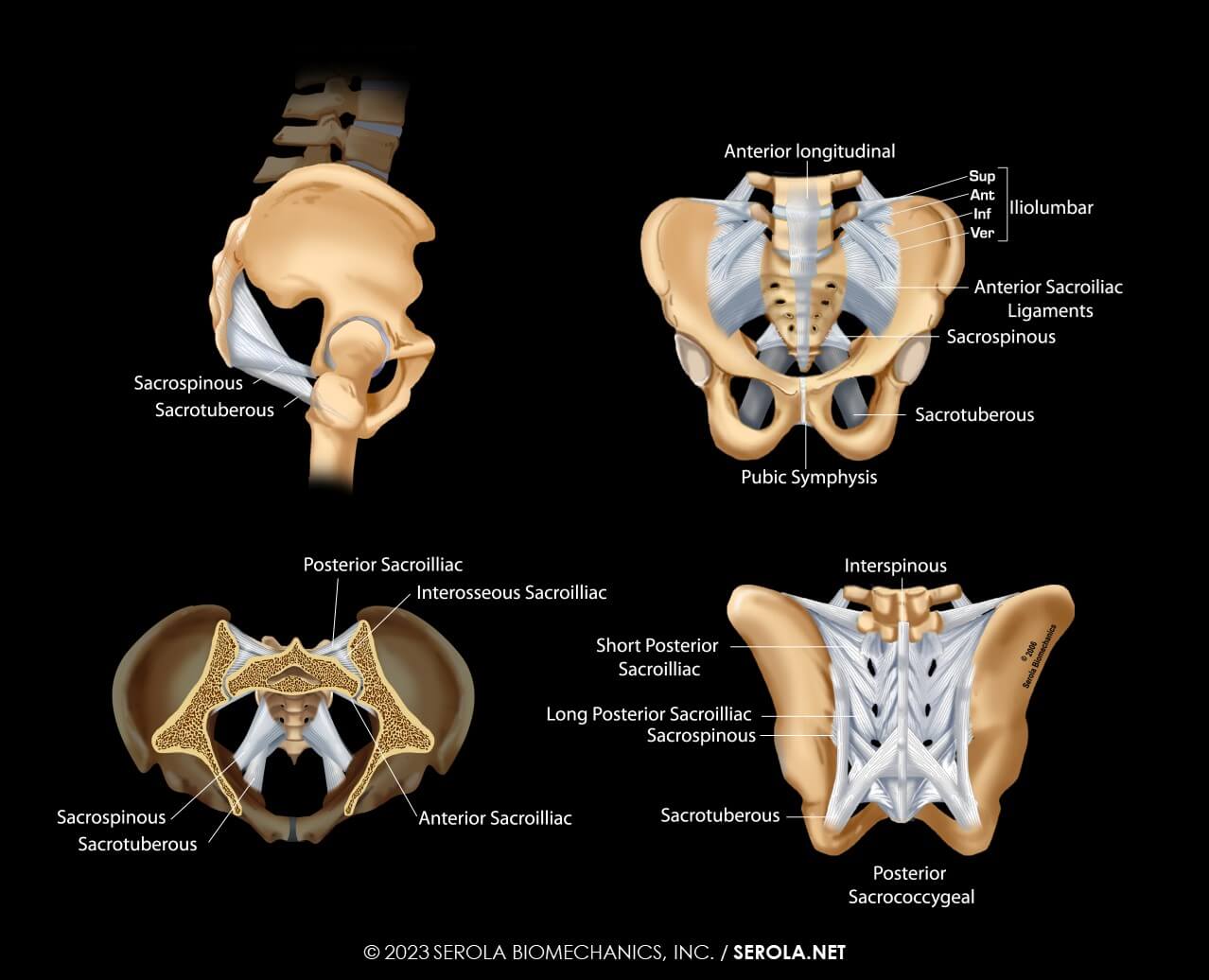
The sacroiliac joint has the strongest ligament system in the body. They are categorized according to their function of limiting nutation or counternutation.
Ligaments limiting nutation include the sacrospinous, sacrotuberous, anterior capsule, anterior sacroiliac ligament, anterior longitudinal ligament, interosseous ligament, and the short posterior ligaments [1]p62-65 [2]p55-60 and the lower bands of the iliolumbar ligament [3]p545[4] p52 [5]p45-46. Ligaments limiting counternutation include the long posterior ligament, lumbar interspinous ligaments, [1] p62-65 [2] p55-60 and the upper bands of the iliolumbar ligament [3]p545 [4]p52.
LIMITING NUTATION
Sacrospinous Ligament:
- Prevents excess posterior movement of the sacral apex (nutation) [6]
- Removal had little effect on sacroiliac joint movement [7]
Sacrotuberous Ligament:
- Prevents posterior movement of the sacral apex [2, 6, 8]
- Limits anterior movement of the sacral base [2, 8] p55-60
- Removal had little effect on sacroiliac joint movement [7]
Anterior Capsule:
- Encapsulates joints and confines synovial fluid within them[9]
- 9-21% of patients with chronic pain below L5-S1 had anterior capsular tears[9]
- Prevents excess nutation
- Regulates muscle tone. Pinching different areas caused proprioceptive reactions involving different muscles [10]
The Anterior Sacroiliac Ligament:
- Blends with fibers of the capsule and is considered to be a thickening of the anterior capsule, which is thin and weak and often tears [6]
- Due to its rich innervation of nociceptive fibers, it may be a significant source of pain.
Anterior Longitudinal Ligament:
- Long, thick ligament that spans the entire length of the spine, from the occiput to the sacrum
- Main function is to limit extension in the spine, which translates to limiting nutation in the sacroiliac joint
The Interosseous Ligament:
- Strongest ligament in the body [11]p434
- Principle ligament that suspends sacrum from ilia
- Prevents excess nutation
- Consists of short, strong bands which do not tear; instead, the fibers detach from the bone [6, 12]
- Fibers blend with those of the posterior capsule [6]
- May interweave to form part of the posterior capsule [13]p16
- Divided into two parts:
- a deep part that is located posterior to the articular portion of the SIJ
- a superficial part that blends with the posterior SI ligament [14]
- Some authors [5]p176 [1]p62 consider the interosseous ligament to be part of the posterior sacroiliac ligaments
- Within the syndesmosis, the interosseous ligament is separated from the posterior SI ligaments by the lateral branches of L5, S1, S2 posterior rami nerves [12] as well as blood and lymph vessels [12, 14]
- Removal of the interosseous ligament had a profound effect on sacroiliac joint movement [7]
The interosseous ligament plays a particularly important role. Vukicevic et al. found that, while removal of the sacrotuberous and/or sacrospinous ligaments did not significantly affect sacroiliac joint motion, removal of the interosseous ligaments had a profound effect. The ilia separated as the sacrum dropped at an angle and fixed between the two ilia. Movement was almost stopped. When the interosseous ligament is intact, its presence prevents tight contact between the articular surfaces of the sacrum and ilia, even when loaded [7]. The space between the ligamentous fibers are filled with nerves, soft areolar connective tissue, fat, elastic tissue, and blood and lymph vessels [6, 12, 14], thereby preventing bone-to-bone contact between the joint surfaces, as incorrectly espoused by promoters of the keystone concept.
The Short Posterior (Dorsal) Sacroiliac Ligament:
- Superior to the posterior superior iliac spine (PSIS) and extends from it and the internal lip of the iliac crest to the intermediate and lateral sacral crests
- Limits nutation by attaching the sacrum to the iliac bones
- Very strong and, with the interosseous ligament, it prevents separation of the sacroiliac joint [2] p55-60
- Some authors [1]p62 [15]p174 consider this ligament to be part of the interosseous ligament
LIMITING COUNTERNUTATION
The Long Posterior (Dorsal) Sacroiliac Ligament:
- Inferior to the PSIS and extends from it and internal lip of the iliac crest to S3-4
- Prevents excessive counternutation [16, 17]
- Slackened when the sacroiliac joints are nutated and tensed when they are counternutated [16] [2]p58 [17]
LIMITING EITHER NUTATION OR COUNTERNUTATION
Iliolumbar Ligaments:
- Composed of bands that run from the articular processes of L4 and L5 to the ilium
- As a group, the iliolumbar ligaments prevent lateral flexion, rotation, extension, and flexion [4, 18], and anterior displacement of L5 on the sacrum [19]p27 [20]
- May originate from muscular fibers that transform into ligaments as one ages [20]
- Limiting Counternutation: lower bands
- From L4, it runs inferiorly to limit spinal flexion (counternutation) [4]p52
- Limiting Nutation: upper bands
- From L5, it runs anteriorly and inferiorly to limit extension (nutation) [4]p52
- Anterior and superior bands from L5 may be derived from fibers of the quadratus lumborum [5]p45-46
- Posterior band of L5 limits flexion (nutation) and may be derived from the iliocostalis lumborum [5] p105 and/or the longissimus lumborum [5]p44
LIMITING NEITHER NUTATION OR COUNTERNUTATION
Axial Sacroiliac Ligament:
The axial sacroiliac joint, situated about 15 mm posterior to the most concave point of the articular part of the SIJ, and anterior to the interosseous ligament, is described by Bakland & Hansen [21] and Bowen & Cassidy [22] as a possible pivot point of SIJ motion.
A great deal of research has been done to identify the center of sacroiliac joint motion, with conflicting results. Wilder, Pope, et al. [23], using surface topography techniques, reviewed the different axes of rotation proposed by Bonnaire, Farabeuf, and Weisl, and found a great deal of variation. They concluded that “The position of the axes of motion varies considerably between individual specimens.”
A brief explanation of the development of the SIJ may help explain why the axial sacroiliac joint appears to be correctly identified as the center of SIJ motion.
The axial sacroiliac joint, situated about 15 mm posterior to the most concave point of the articular part of the SIJ, and anterior to the interosseous ligament, is described by Bakland & Hansen [21] and Bowen & Cassidy [22] as a possible pivot point of SIJ motion.
Developmentally, until the late teens, the sacroiliac joint is smooth and flat such that a gliding motion can occur in all directions [22]. By the early twenties, the iliac surface develops a ridge running down the middle of the two wings. At the same time, the sacral surface develops a corresponding groove into which the iliac ridge glides. Following the development of this ridge and groove the sacroiliac joint appears to move in a linear fashion along this track. Soon afterwards, a bony tubercle, known as the axial sacroiliac joint, develops on the ilium, with a corresponding depression on the sacrum, just posterior to the articular portion of the sacroiliac joint. The fact that this joint develops soon after the ridge and groove supports the idea that it is associated with the SIJ’s movement. Bakland& Hansen[21], as well as Bowen & Cassidy [22, and Bechtel {Bechtel, 2001 #233] believe that this joint functions as the center of SIJ motion. Kapandji [1] also mentions that, according to the classical theory of Farabeuf, the axial joint was described as the center of motion of the SIJ.
Bakland & Hansen [21] found that, within the axial sacroiliac joint is the axial interosseous ligament (AIL), which, at 3.2cm2, makes up 14% of the total syndesmosis area and has its own capsule and synovial membrane. In agreement, Bechtel [24] measured it at 2.9cm2 but only in women, whose area would be expected to be slightly smaller. The remaining 86% of the syndesmosis is the sacroiliac interosseous ligament (SIL). However, where the SIL is one of the strongest ligaments in the body, the AIL is one of the weakest, as measured by failure load and failure stress, due to the low ratio of collagen and high ratio of connective tissue and blood vessels (only the ligamentum flavum is weaker). With this knowledge, Bechtel proposed that, since the AIL is at the center of motion of the SIJ, structural strength would not be needed since it does not function as a mechanical restraint; rather, it may serve a proprioceptive role.
So, while the ilia appear to rotate about the center of each acetabulum, the sacrum appears to pivot about the two axial sacroiliac joints simultaneously. As a pivot point, it would be the center of motion, like a fulcrum on a teeter-totter, but because the axial joint is non-weight bearing, the motion must be generated by a pulling action on either side of the fulcrum, rather than by compression. Other ligaments would prevent separation, whereas the axial ligament mainly, or only, provides proprioceptive feedback.
It appears that the sacrum, instead of rotating, pivots about one axial sacroiliac joint on each side in a rocking motion. For this pivoting to occur, there must be numerous attachment points to the ilium on each side, which pull the sacrum through its range of motion. It is evident that there are plenty of ligaments surrounding the axial sacroiliac joint, including the interosseous and capsular ligaments, to provide the necessary pulling action. For more, please see Facets Curl Around the Sacrum.
References:
1. Kapandji, I.A., The Physiology of the Joints. Vol. 3. 1977: Churchill Livingstone.
2. Vleeming, A., et al., The role of the sacroiliac joints in coupling between spine, pelvis, legs and arms., in Movement, Stability, and Low Back Pain, A. Vleeming, et al., Editors. 1997, Churchill Livingstone. p. 53-71.
3. Oatis, C.A., Kinesiology. The Mechanics and Pathomechanics of Human Movement. 2004: Lippincott Williams & Wilkins.
4. Calais-Germain, B., Anatomy of Movement, ed. S. Anderson. 1993, Seattle, WA: Eastland Press.
5. Bogduk, N., Clinical Anatomy of the Lumbar Spine and Sacrum. 2005: Elsevier Churchill Livingstone.
6. Sashin, D., A critical analysis of the anatomy and the pathologic changes of the sacro-iliac joints. The Journal of Bone and Joint Surgery, 1930. 12: p. 891.
7. Vukicevic, S., et al., Holographic analysis of the human pelvis. Spine, 1991. 16(2): p. 209-14.
8. Vleeming, A., et al. Load Application to the Sacrotuberous Ligament: Influences on Sacroiliac Joint Mechanics. in Proceedings of the First Interdisciplinary World Congress on Low Back Pain And its Relation to the Sacroiliac Joint. 1992. Rotterdam: ECO.
9. Schwarzer, A.C., C.N. Aprill, and N. Bogduk, The sacroiliac joint in chronic low back pain. Spine, 1995. 20(1): p. 31-7.
10. Indahl, A., et al., Sacroiliac joint involvement in activation of the porcine spinal and gluteal musculature. Journal of Spinal Disorders, 1999. 12(4): p. 325-30.
11. Haldeman, S., et al., eds. Principles and Practice of Chiropractic. 3rd ed. 2005, McGraw-Hill.
12. Grieve, G.P., The sacro-iliac joint. Physiotherapy, 1976. 62(12): p. 384-400.
13. Willard, F.H., The muscular, ligamentous, and neural structure of the low back and its relation to back pain, in Movement, Stability, and Low Back Pain. The essential role of the pelvis., A. Vleeming, et al., Editors. 1997, Churchill Livingstone: New York, NY. p. 3-25.
14. Rosatelli, A.L., A.M. Agur, and S. Chhaya, Anatomy of the interosseous region of the sacroiliac joint. The Journal of Orthopaedic and Sports Physical Therapy, 2006. 36(4): p. 200-8.
15. Levangie, P. and C. Norkin, Joint Structure and Function. A Comprehensive Analysis. 2005, Philadelphia, PA: F.A. Davis Company.
16. Vleeming, A., et al., The function of the long dorsal sacroiliac ligament: its implication for understanding low back pain. Spine, 1996. 21(5): p. 556-62.
17. Pool-Goudzwaard, A.L., et al., Insufficient lumbopelvic stability: a clinical, anatomical and biomechanical approach to ‘a-specific’ low back pain. Man Ther, 1998. 3(1): p. 12-20.
18. Yamamoto, I., et al., The role of the iliolumbar ligament in the lumbosacral junction. Spine (Phila Pa 1976), 1990. 15(11): p. 1138-41.
19. Adams, M.A., et al., The Biomechanics of Back Pain. 2002: Churchill Livingstone.
20. Luk, K.D., H.C. Ho, and J.C. Leong, The iliolumbar ligament. A study of its anatomy, development and clinical significance. The Journal of Bone and Joint Surgery. British volume, 1986. 68(2): p. 197-200.
21. Bakland, O. and J.H. Hansen, The “axial sacroiliac joint”. Anatomia Clinica, 1984. 6(1): p. 29-36.
22. Bowen, V. and J.D. Cassidy, Macroscopic and microscopic anatomy of the sacroiliac joint from embryonic life until the eighth decade. Spine, 1981. 6(6): p. 620-8.
23. Wilder, D.G., M.H. Pope, and J.W. Frymoyer, The functional topography of the sacroiliac joint. Spine, 1980. 5(6): p. 575-9.
24. Bechtel, R., Physical characteristics of the axial interosseous ligament of the human sacroiliac joint. Spine J, 2001. 1(4): p. 255-9.