
Gluteus Max. – Latissimus Dorsi Muscle Sling
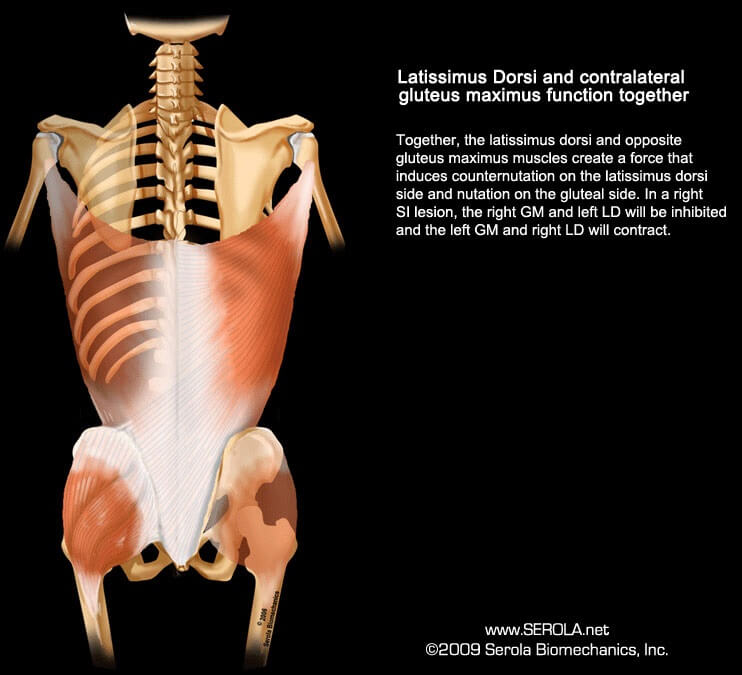
Together, the latissimus dorsi (LD) and opposite gluteus maximus (GM) muscles create a force that induces nutation on the gluteal side and counternutation on the latissimus dorsi side. In a right SI lesion, the left GM and right LD will contract, and the right GM and left LD will be inhibited.
At the level of L4 to L5, the lumbodorsal fascia is not connected to either the spine or ligaments. Instead, these free fibers mesh with fibers of the latissimus dorsi and superior division of the contralateral gluteus maximus to provide a coupling action [1-3] [4]p129
Proponents of the keystone concept believe that this force couple can assist in sacroiliac joint stability by providing a force that is relatively perpendicular to the joint surface. Because these muscles are inhibited in a sacroiliac injury, they assumed that dysfunction in the muscles preceded sacroiliac joint instability; however, they offer no explanation of how the muscles became dysfunctional. On the other hand, the Serola Musculoskeletal Integration Theory, being based on the ligamento-muscular reflex, states that sacroiliac ligament injury precedes muscle dysfunction (see Mechanisms of Injury and Muscular Adaptations). An injury to the joint will cause reflexive muscular reactions.
Gracovetsky [5] describes this coupled action of the latissimus dorsi, through the lumbodorsal fascia to the gluteus maximus, as a key component of energy transfer in gait. A lateral bending movement in the spine is converted into axial torque that drives pelvic rotation. Through this mechanism, energy is transmitted between the upper extremities and legs.
In a relatively normal SIJ, combining Color Doppler Imaging with oscillation, Wingerden [3] showed that the gluteus maximus, along with the erector spinae and the biceps femoris, produced a significant increase in sacroiliac joint stiffness, along with a lesser, but similar, effect from the contralateral latissimus dorsi. We can assume that these muscles produced a nutation effect on the gluteal side since, during nutation, the joint surfaces approach each other as the interosseous ligament winds tighter and the joint may become more stable.
Good Study, Bad Interpretation
As happens too often in the literature, although a study’s methodology is done well, the interpretation of the results may be mistaken by people with pre-conceived concepts. In a certain study, Mooney et al. [7] did an EMG study on patients with confirmed sacroiliac joint dysfunction. On patients with right painful sacroiliac joints, they found hyper-activity of the right gluteus maximus during left trunk rotation, which would induce nutation at the right sacroiliac joint. As a result, they concluded that one significant finding of their study is that the gluteus maximus is hyper-active in sacroiliac joint dysfunction when stress is applied to the sacroiliac joint during strengthening. They apparently misinterpreted this hyperactivity as an indication that the gluteus maximus was trying to stabilize the sacroiliac joint dysfunction. They also found the contralateral latissimus dorsi to be concurrently hypoactive. Exercise to both muscles resulted in increased tone to the latissimus dorsi and decreased tone to the gluteus maximus, with a reduction in pain. In other words, they incorrectly indicate that the normal gluteus maximus/latissimus dorsi coordination does not work when the sacroiliac joint is in lesion. At first glance, this finding does not agree with the nutation lesion concept that both the ipsilateral gluteus maximus and contralateral latissimus dorsi are inhibited in sacroiliac joint dysfunctions.
However, with a different interpretation of the results, it appears that what actually happened does fit into the model of the nutation lesion. The compensating pattern of counternutation should have caused anterior pelvic tilt, facet jamming at L4 to S1, and narrowing of the lateral canals. The narrowed canals most likely led to compressive irritation of the inferior gluteal nerve (L5 to S2), causing gluteus maximus hyperactivity. Left trunk rotation increased the right lumbar lordosis [5], further narrowing the lateral canals and increasing pressure on the nerve roots. The opposite latissimus dorsi was not involved because it is fed by the thoracodorsal nerve from C6 to C8. The left latissimus dorsi was hypotonic, as the right gluteus maximus would have been if not for the extra complication of irritation to the nerve roots.
Interestingly, their study showed that exercise to both muscles increased tone to the latissimus dorsi and decreased tone to the gluteus maximus; this is the clue that leads to understanding the apparent incongruity. It appears that the superior division of the gluteus maximus, is a pelvic extensor, when strengthened, eventually created enough posterior rotation of the pelvis that it was able to decrease the acute angulation at the lumbosacral area and decompress the lateral canals. The pressure on the inferior gluteal nerve was removed and normal tone, or even hypotonia (because the ipsilateral sacroiliac joint was in lesion), was restored to the gluteus maximus. Although post-exercise, left torso rotation increased lordosis, as it did pre-exercise, the lateral canals may have opened enough to allow the lordosis to occur without pressing on the nerve roots.
This is a good example of a compensation-to-a-compensation pattern. Having a good understanding of the underlying patterns, as expressed in the Musculoskeletal Integration Theory, can greatly assist one in making sense out of disparate findings.
References:
1. Snijders, C.J., Transfer of Lumbosacral Load to Iliac Bones and Legs: Part 2 – Loading of the Sacroiliac Joints when Lifting in a Stooped Position. Clinical Biomechanics, 1993b. 8: p. 295-301.
2. Vleeming, A., et al., The role of the sacroiliac joints in coupling between spine, pelvis, legs and arms., in Movement, Stability, and Low Back Pain, A. Vleeming, et al., Editors. 1997, Churchill Livingstone. p. 53-71.
3. Wingerden, J.v., et al. Muscular Contribution to Force Closure: Sacroiliac Joint Stabilization In Vivo. in 4th Interdisciplinary World Congress on Low Back & Pelvic Pain. 2001.
4. Adams, M.A., et al., The Biomechanics of Back Pain. 2002: Churchill Livingstone.
5. Gracovetsky, S. Locomotion – Linking the Spinal Engine with the Legs. in Proceedings of the Second Interdisciplinary World Congress on Low Back Pain. 1995. San Diego, CA.
6. Vleeming, A., et al., The function of the long dorsal sacroiliac ligament: its implication for understanding low back pain. Spine, 1996. 21(5): p. 556-62.
7. Mooney, V., et al., Coupled motion of contra lateral latissimus dorsi and gluteus maximus-its role on sacroiliac stabilization, in Movement, Stability, & Low Back Pain, A. Vleeming, et al., Editors. 1997, Churchill Livingstone. p. 115-122.